

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are my main takeaways I would share with you as a friend:
- Thyroid disorders, including hypothyroidism and hyperthyroidism as well as thyroid antibodies commonly contribute to miscarriage and infertility.
- This article discusses these conditions, how they relate to fertility and an in-depth look at treatment options.
- Women with thyroid conditions can have their condition under control and maintain healthy pregnancies.
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
Table of Contents
How thyroid disorders affects fertility and pregnancy
Hypothyroidism
Hyperthyroidism
Thyroid antibodies
Conventional treatments for hypothyroidism
Conventional Treatments for Hyperthyroidism
Experimental and alternative treatments for thyroid conditions
Healthy thyroid function is critical for pregnancy. Therefore, thyroid disorders such as hypothyroidism, hyperthyroidism, and autoimmunity can cause infertility and miscarriage.
Keep in mind that:
- Thyroid disorders can be hidden. It is possible to have it and be completely unaware.
- 15% of premenopausal women have thyroid antibodies, even with normal TSH and T4 1.
- Thyroid antibodies are found in 17 – 33% of women with recurrent miscarriages 23.
- A pregnancy or previous miscarriage can trigger thyroid disorder or autoimmunity.
Read part 1, linked here, of this 2-part article, where we covered thyroid lab tests. In this article, part 2, we cover everything you need to know about thyroid disorders and autoimmunity.
How thyroid disorders affects fertility and pregnancy
The thyroid hormones stimulate oocyte development, ovulation, and menstrual cycle. If you have too high or too low thyroid function, you may experience irregular cycles 4.
The thyroid hormones control 5:
- Sex hormone production
- Levels of sex hormone-binding globulin, which binds sex hormones in the blood
- Chemical breakdown or deactivation of sex hormones
Therefore, both too little and too much thyroid can contribute to sex hormone imbalances leading to irregular cycles, difficulty conceiving, and miscarriages.
Thyroid disorders can also increase oxidative stress, which may affect fertility and pregnancy 67.
Abnormal thyroid hormones, despite normal thyroid function, are also associated with Polycystic Ovarian Syndrome (PCOS) 8. Read more on PCOS, linked here. Also, women with PCOS are more likely to have subclinical hypothyroidism 9.
During pregnancy – Your thyroid hormone function increases significantly during the first trimester and drops during later trimesters. The thyroid hormones control placental tissue development. In the first trimester, it also produces the hormones for both the mother and the fetus before the fetus can produce its own thyroid hormones. The increased need for thyroid function and thyroid hormone production during pregnancy also explains the increased need for iodine during pregnancy 10.
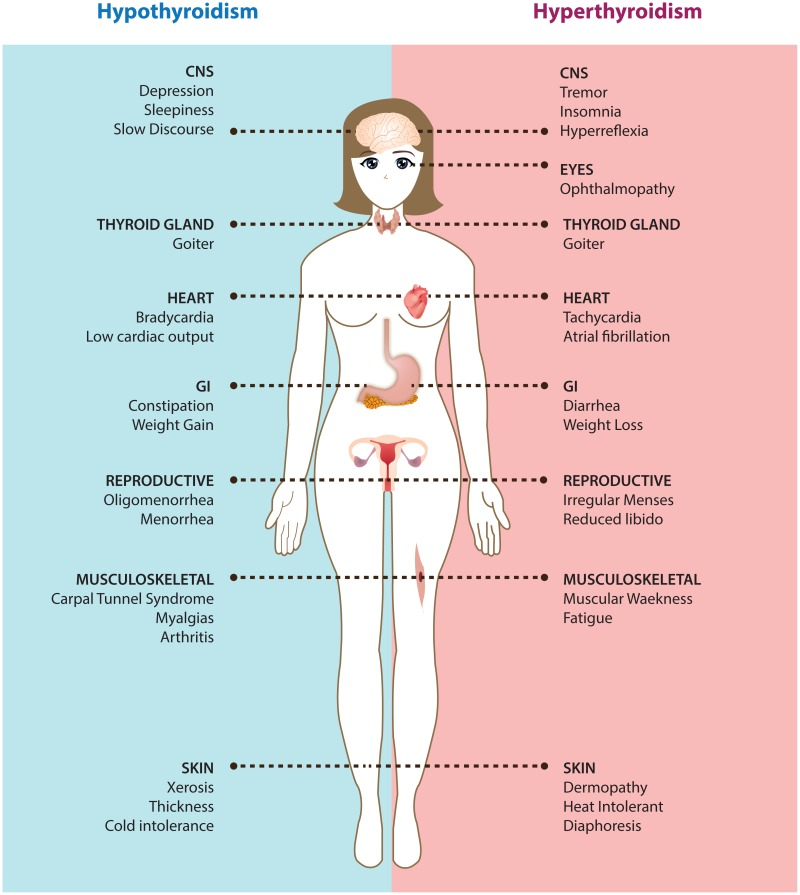
Hypothyroidism
Hypothyroidism is a disease of reduced thyroid function. In countries with iodine added to salt, the most common form of hypothyroidism is Hashimoto’s thyroiditis, due to having antibodies that attack the thyroid. In countries without salt iodization, the most common form of hypothyroidism is due to iodine deficiency goiter.
Typical symptoms of hypothyroidism include fatigue, constipation, being cold, depression, dry skin, slower heart rate, weight gain, and menstrual irregularities.
Hypothyroidism is diagnosed when TSH levels are above normal and fT4 levels are below normal. These reference values vary from trimester to trimester and are also different in non-pregnant women.
Table: Lab cutoff values for the diagnosis of hypothyroidism
| Tests | Nonpregnant | First trimester | Second trimester | Third Trimester |
| TSH (mIU/L) | >4.3 | >2.5 | >3.0 | >3.0 |
| Free T4 (ng/dL) | <0.8 | <0.8 | <0.6 | <0.5 |
Hyperthyroidism
Hyperthyroidism is when you have too much thyroid hormones. Grave’s disease is the most common, but not the only form, of hyperthyroidism. It is an autoimmune disorder where thyroid antibodies stimulate the TSH receptor function, resulting in excessive thyroid hormones 12.
Hyperthyroidism may cause ovarian cysts and increase the death of follicles 13. Women with hyperthyroidism may experience anxiety, insomnia, diarrhea, shakiness, heat intolerance, fast heart rate, hair loss, sweaty skin notably on the palms, and fast weight loss and menstrual cycle disorders.
Hyperthyroidism is diagnosed when TSH levels are below normal and fT4 levels are above normal. These reference values vary from trimester to trimester and are also different in non-pregnant women.
Table: Lab cutoff values for the diagnosis of hyperthyroidism
| Tests | Nonpregnant | First trimester | Second trimester | Third Trimester |
| TSH (mIU/L) | <0.3 | <0.1 | <0.2 | <0.3 |
| Free T4 (ng/dL) | >1.7 | >1.2 | >1.0 | >0.8 |
Thyroid antibodies
Having thyroid antibodies is a disorder of the immune system rather than the thyroid itself. These antibodies may target proteins of the thyroid or proteins that affect thyroid hormone function.
Table: Different thyroid antibodies, their effects on thyroid function, and thyroid conditions found
| Protein attacked by antibodies | Antibody names and synonyms | Effects | Found in |
| Thyroglobulin (Tg) | Thyroglobulin antibodies (TgAb) | Nothing or thyroid inflammation and destruction | Hashimoto’s |
| Thyroperoxidase (TPO) | Thyroperoxidase antibodies (TPOAb) | Nothing or thyroid inflammation and destruction | Hashimoto’s |
| TSH receptor (TSHR or TR) | TSH receptor antibodies (TSHRAb or TRAb)Thyroid stimulating immunoglobulin (TSI) | May stimulate, block, or do nothing to TSH receptors, depending on the case. | Grave’s, Hashimoto’s, and Atrophic thyroiditis |
TPOAb is generally more problematic, and more common in Hashimoto’s and postpartum thyroiditis. Some people with normal thyroid function have TgAb and TPOAb, whereas TSHRAb is only found in Grave’s and some Hashimoto’s patients 14.
Thyroid antibodies are naturally highest during the first trimester and decline throughout the pregnancy, but significantly increase again postpartum. Women with thyroid antibodies are at higher risk of developing hypothyroidism or hyperthyroidism, especially postpartum. This is called postpartum thyroiditis.
Note: Thyroglobulin is a protein that is part of the thyroid gland, which is different from thyroxine-binding globulin. Thyroxine-binding globulin (TBG) is a protein that binds to thyroid hormones outside the thyroid and helps transport them through the blood.
The antibodies can attack and destroy the thyroid tissue, resulting in declining thyroid function over time. People who have antibodies are more likely to develop full-on thyroid disorders upon triggers. In women, pregnancy and menopause are common triggers due to the changes in the immune system and hormones 15. However, the antibodies can also spontaneously disappear 16.
A large-scale meta-analysis involving 12,126 women found that thyroid antibodies were associated with a four times higher risk of miscarriage 17. Thyroid antibodies are also associated with increased IVF failure rates and miscarriage risks among pregnancies from IVF 18. In both natural and assisted pregnancy, the treatment of women with thyroid antibodies with levothyroxine cuts miscarriage rates by half 1920.
Therefore, thyroid antibodies may indicate a high-risk pregnancy, although many women with thyroid antibodies can have successful pregnancies without any treatment 21.
We still don’t know why thyroid antibodies cause miscarriage. Potential reasons why thyroid antibodies may lead to miscarriages include 22:
- Subtle hypothyroidism due to the antibodies
- The coexisting autoimmune imbalance or other autoimmune conditions during the pregnancy
- The thyroid antibodies may interfere with the placenta or fertilized egg, resulting in a rejection
- Thyroid antibodies increase with age, which also correlates with infertility and pregnancy complications
During a pregnancy, TPOAb also increases the risk of placental abruption and preterm delivery 2324.
What causes thyroid antibodies?
Similar to antiphospholipid syndrome, having thyroid antibodies is a sign of ongoing autoimmunity. There is no one cause, but rather multiple contributing factors that trigger thyroid antibodies.
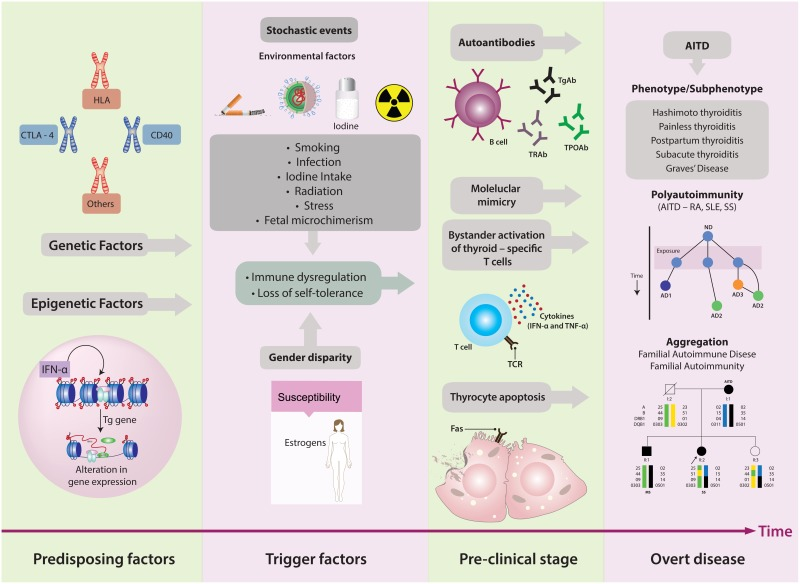
Risk factors for having thyroid antibodies include:
- Female gender – women are 18 times more likely to develop thyroid autoimmunity than men 26
- Genetics – there is not one gene but multiple genes that contribute to thyroid disorders. These genes control immune function or tolerance, such as Human Lymphocyte Antigen (HLA) genes and genes that control inflammation. Genes that provide instructions to produce Tg and TSHR proteins are also linked to autoimmune thyroid diseases 27. Thyroid disorders tend to run in the family 28.
- Lifestyle or environmental factors causing loss of self-tolerance, such as:
- Radiation exposure
- Stress and traumas
- Excessive iodine intake
- Toxic exposure, such as pollution, plastic residues, and pesticides 29
- Infections, such as Helicobactor pylori (the bacteria that causes stomach ulcers), Borrelia burgdorferi (implicated in Lyme’s disease), Yersinia enterocolitica, Coxsackie virus, and retroviruses 30
- Other triggers of immune activation, such as gluten sensitivity and Celiac disease 31
- Medications such as lithium, Interferon-alpha, Highly Active Antiretroviral Therapy for HIV, amiodarone 32
- Having other autoimmune diseases (polyautoimmunity) – having one autoimmunity significantly increases your risk of developing another 33. Women with TPO antibodies are also more likely to have antiphospholipid syndrome antibodies 34. For more on antiphospholipid syndrome, see this article.
- Fetal microchimerism is an unproven hypothesis that the fetal cells may graft on the mother’s thyroid, causing the mother’s immune system to attack the thyroid after pregnancy 35.
If you have other autoimmune diseases, family members with thyroid disorders, or used one of the medications above, you should be regularly screened for thyroid disorders 36.
Table: Changes in thyroid function during pregnancy for normal pregnancy, and in women with hypothyroidism and hyperthyroidism 37
| Maternal thyroid status | TSH | Free T4 | Total T4 | Free T3 | Total T3 | Free T3 index | T3* uptake |
| Normal thyroid function | Decrease | No change | Increase | Increase | Increase | No change | Decrease |
| Hypothyroidism | Increase | Decrease | Decrease | Decrease/no change | Decrease/no change | Decrease | Decrease |
| Hyperthyroidism | Decrease | Increase | Increase | Increase/no change | Increase/no change | Increase | Increase |
*T3 uptake is a measure of TBG level, which indicates the percentage of thyroid-binding globulin in blood samples.
Conventional treatments for hypothyroidism
Thyroid hormone replacement is the standard treatment for hypothyroidism. Currently, there is no specific conventional treatment to reduce thyroid antibodies in patients with normal thyroid function. Fortunately, studies have shown that some alternative and experimental treatments may reduce thyroid antibodies (see the next section).
T4 (Levothyroxine)
Levothyroxine (LT4 or Synthroid), a synthetic thyroxine (T4), is the standard treatment for hypothyroidism. It allows the target tissues to convert the T4 into T3 naturally, allowing your body to adjust for the required T3 levels. It is also better absorbed through the gut than liothyronine and has a longer half-life, making it possible to dose only once a day.
The daily dose of levothyroxine depends on age, gender, and body size. A starting dose for subclinical hypothyroidism (TSH under 10 mIU/L) is between 25 – 75 mcg. Your doctor may titrate the dosage up until your TSH falls below 2.5 mIU/L for preconception. The full thyroid replacement dosage is 0.73 mcg/lb or 1.6 mcg/kg body weight 38.
Levothyroxine should be taken on an empty stomach first thing in the morning and away from medications and supplements that may interfere with its function. Then, wait 30 – 60 minutes to eat. Iron supplements, calcium supplements, and soy products may interfere with levothyroxine absorption and usage.
If you have pre-existing hypothyroidism, your doctor may adjust your thyroid dose as soon as you become aware of the pregnancy. This will provide sufficient thyroid hormones to the fetus, especially during the first trimester.
Up to 70% of hypothyroid women will require at least a 30% increase in their thyroid medications during early pregnancies 39.
T3 (Cytomel)
Liothyronine (LT3 or Cytomel) is the synthetic version of T3. When the patient still experiences symptoms even with LT4 treatment, some endocrinologists may prescribe Cytomel to raise T3 levels. A typical dosage for this is approximately 1/13 to 1/20 the dose of LT4 40.
While some hypothyroid patients may do better with a combination of Cytomel and Levothyroxine treatments, evidence for LT3 safety and effectiveness is limited 41. LT3 also does not cross the placenta.
Desiccated thyroid extract
Desiccated thyroid is the dried and powdered thyroid gland from animals such as pigs or cows. It is the oldest hypothyroidism treatment available. Some doctors may consider it obsolete as the synthetic thyroid hormones are more consistent. However, many patients feel better on desiccated thyroid, which contains not only the thyroid hormones but also calcitonin, thyroid cofactors, and their metabolites. Common brands include Armour and Naturethroid.
The dosage of desiccated thyroid is in “grains,” where each grain contains 60 – 65 mg of the medication. It typically contains around 38 mcg of T4 and 9 mcg of T3 42.
In a blinded study of 70 hypothyroid patients, 49% of them preferred the desiccated thyroid, 19% preferred levothyroxine, whereas 23% had no preference. Symptom scores, however, did not change significantly between groups 43.
Conventional Treatments for Hyperthyroidism
For hyperthyroidism, thyroid-suppressing drugs, radioactive iodine, and surgery are options to reduce thyroid function. These patients may need hypothyroidism treatments after a thyroid ablation radioactive iodide treatment or surgery to permanently correct thyroid function.
It is important to tell your physician about past or ongoing Grave’s disease if you are pregnant. Even if the condition is well-managed, you may still have the antibodies, which can affect the pregnancy. Also, if you are on Carbimazole, you should speak to your doctor about switching to propylthiouracil as soon as you become pregnant. Propylthiouracil is the best option for preconception and early pregnancy. Also, it is important to get regular checkups if you have Grave’s disease during pregnancy.
Beta blockers
Once your doctor finds elevated thyroid function, they may prescribe a beta-adrenergic receptor blocker (beta blocker). These are heart disease drugs used off-label to block the conversion of T4 to T3 at high doses. Propranolol (10 – 40 mg, 3 – 4 times a day) may be prescribed for nursing and pregnant mothers.
Radioactive iodine 4445
Radioactive iodine is not safe for pregnancy, so the treatment should be completed at least 6 months before conception. It is also contraindicated during breastfeeding, so it is not offered to new mothers.
The thyroid gland uses iodine to produce T3 and T4, When the thyroid gland uptakes the radioactive iodine, the radiation destroys the overactive thyroid cells. You can take the medication orally as prescribed every month until the thyroid gland shrinks and symptoms lessen. This treatment usually takes 1 – 2 months and the thyroid function should stabilize in about 8 – 12 weeks.
The desired result of radioactive iodine treatment is hypothyroidism. After that, you will be prescribed medications for hypothyroidism to maintain normal thyroid hormone levels. This treatment modality is still preferred to other hyperthyroidism treatments, especially in young people, due it’s fewer relapse frequency.
If you take antithyroid drugs, you should discontinue them preferably 2 weeks before radioiodine treatment, or at least 2 days prior to taking the radiopharmaceutical.
Your clinic will also inform you of other precautions to protect others from the radioactive iodide during this treatment. This includes avoiding prolonged close contacts with other people, and separating linens, dishes and bathrooms whenever possible.
Thyroid surgery 4647
In some medication-resistant hyperthyroidism or thyroid tumors, surgery may be necessary. There are a few approaches depending on how much tissue needs to be removed:
- An isthmusectomy – removal of just the bridge of thyroid tissue between the two lobes;
- A hemithyroidectomy or thyroid lobectomy – one lobe (one half) of the thyroid is removed;
- A total thyroidectomy – removal of all or most of the thyroid tissue.
Risks that arise from this procedure are minimal but include: infection, bleeding, nervus laryngeus recurrens injury (which disturb the voice production), parathyroid glands injury as well as complications that are associated with general anesthesia.
Before the surgery, your doctor will perform a workup, such as blood tests (CBC and biochemistry, hormonal levels, cytology results), chest X-ray, and ECG as well as thyroid ultrasound exam. Don’t forget to tell your doctor if you take blood thinners. They may advise you to stop the medication before the procedure.
During the surgery, you are under general anesthesia, and it usually lasts around 2 hours. After the procedure, the surgeon will stitch the incision on your neck that is usually a few inches long. The stitches are held for around two weeks. If you notice inflammation, redness, pain, swelling, fever, or odd smell, contact your physician. At first, you will take liquid food, but as soon as the next day you can start eating normally and go home.
Methimazole and Propylthiouracil
Most providers treat hyperthyroid pregnant women with antithyroid medicines called propylthiouracil in the first trimester and methimazole in the second and third trimesters. The timing of these medicines is important. Propylthiouracil after the first trimester can lead to liver problems. Methimazole in the first trimester may increase the risk of birth defects.
For pre-existing Grave’s disease, your doctor may prescribe the lowest possible dose of propylthiouracil (50 – 100 mg every 8 hours) and recheck with a blood test every 3 – 4 weeks. Propylthiouracil crosses the placenta. It may cause goiter and hypothyroidism in the fetus.
Experimental and alternative treatments for thyroid conditions
The following experimental treatments may help with thyroid conditions although there is limited evidence for their safety and effectiveness. However, stress management, a healthier lifestyle, and correcting nutrient deficiencies are generally applicable to improving all pregnancy outcomes.
Intravenous Immunoglobulin (IVIG)
Intravenous Immunoglobulin (IVIG) is an antibody that ties up autoimmune antibodies, such as the thyroid antibodies. Based on small clinical studies, IVIG may prevent the antibodies from interfering with fertility and pregnancy. As a result, many women who previously had multiple miscarriages were able to achieve full-term pregnancies.
In a study of 47 women with recurrent miscarriages, 20 of them continued the IVIG, and 19 of them carried the pregnancy to term. Seven of the 11 women who declined IVIG in this study became pregnant but all miscarried 48.
In another study of 37 women with recurrent miscarriages and thyroid antibodies – 11 were treated with IVIG and 16 on levothyroxine. 5 of the women with IVIG treatments achieved full-term pregnancies, whereas 15 women with antibodies treated with levothyroxine achieved full-term pregnancies. Based on this small sample, it is likely that levothyroxine was more effective than IVIG at preventing miscarriage 49.
Dietary Treatments
A gluten-free diet may reduce antibodies in women with elevated antibodies and subclinically elevated TSH. A study involved 34 women with TPOAb and TgAb, and subclinically elevated TSH levels. After 6 months on a gluten-free diet, antibodies significantly decreased, while TSH slightly decreased and thyroid hormones slightly increased 50.
Another study enrolled 17 women with Hashimoto’s thyroiditis to participate in a 10-week online health coaching program following the Autoimmune Paleo Protocol diet. The program also promoted sleep hygiene, stress management, support system, and increased outdoor activities. The inflammation marker hsCRP decreased, but thyroid antibodies and thyroid hormone levels did not significantly change. The participants also experienced significantly improved quality of life 51.
Low-dose naltrexone
Naltrexone🅧 is a drug that blocks opiate receptors now often used off-label to treat inflammatory and autoimmune diseases. Recently, many clinical trials have evaluated its safety and effectiveness for other autoimmune diseases 52. While there is very limited evidence, anecdotally, many Hashimoto’s and Grave’s patients experience significant improvement in their quality of life after introducing very low doses of naltrexone. If you will introduce low-dose naltrexone (LDN) as part of your treatment protocol, it is important to work with a physician and a compounding pharmacist who are familiar with the drug. Also, since your other thyroid medications may need to be adjusted, do not introduce LDN without first speaking to your doctor. Due to limited data on the safety and effectiveness of this drug, it is not recommended during pregnancy.
Dietary Supplements and Nutrients
Selenium – Selenium is a trace element with many important roles in thyroid function. In patients with high TPOAb from areas of low selenium, 200 mcg of supplementation reduced TPOAb 5354. Among pregnant women, 200 mcg of selenomethionine supplementation significantly reduced the rate of autoimmune thyroiditis, postpartum thyroid disorders, and permanent hypothyroidism compared to placebo 55.
Vitamin D – Many hypothyroid and autoimmune patients also have low vitamin D 56. Both low vitamin D and autoimmunity can contribute to miscarriage, so it is a good idea to maintain healthy vitamin D levels. To learn more about this, see our vitamin D article.
Addressing anemia – Iron is an important mineral both for general health and pregnancy. Pregnant women who have hypothyroidism and thyroid antibodies are more likely to develop iron-deficiency anemia 57. It is, therefore, important to monitor your bloodwork to ensure that you are consuming enough iron both preconception and during pregnancy.
Stress reduction
Based on a small study involving 60 women with Hashimoto’s, an 8-week stress reduction program improved quality of life, reduced thyroid antibodies, and improved thyroid function 58.
Conclusion
If you have had miscarriages, it is important to rule out thyroid disorders and antibodies. These can also make it harder to get pregnant. Also, if you have PCOS and other autoimmune conditions, you should get screened for thyroid disorders. Fortunately, there are very effective treatments and natural ways to support your thyroid function so that you can achieve a full-term healthy pregnancy.
Next Steps to Consider
- If you are experiencing infertility or miscarriage, make sure to have your thyroid levels tested (learn more about testing in this article).
- If you do have issues with your thyroid levels, discuss the above diet, lifestyle and treatment options with your doctor or health care professional.
- Stay hopeful! Women diagnosed with both hyperthyroid and hypothyroid can go on to have a successful pregnancy.
References

0 Comments