

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are my main takeaways I would share with you as a friend:
- The majority of early miscarriages are due to genetic causes.
- This article discusses, in-depth, genetic tests that are available to you, before and during pregnancy as well as after a miscarriage.
- Work with your doctor or other health care professional to help determine testing that will be the best fit for you.
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
Table of Contents
Purposes of Genetic Tests
Screening vs Diagnostic
Parental Screening
Prenatal (Pregnancy) Genetic Screening
Preimplantation genetic tests with IVF
Product of conception genetic tests
Genetic Testing Technologies for Miscarriage
Karyotype Analysis
Fluorescent in situ Hybridization
Comparative Genomic Hybridization (CGH)
Chromosomal Microarray
Next-generation sequencing
Polymerase Chain Reaction
Most early miscarriages are due to genetic causes, including chromosomal abnormalities, although over 50% of cases have no identified causes. Genetic testing can provide closure and potentially critical information to improve your chance of success in future pregnancies. Recent technologies, such as chromosomal microarray and next-generation sequencing, have made it easier and more affordable to understand the reasons behind miscarriages. In our genetic causes and chromosomal abnormalities article, we covered different types of genetic anomalies that can cause miscarriages. In this article, we will cover different testing options, purposes of each test, and whether you should get genetic testing.
Purposes of Genetic Tests
Genetic tests are medical tests that identify changes in chromosomes, genes, or proteins. Some tests determine genetic sequences, while others only look for known genetic variants. It could be done in either parent, embryo, or fetus.
Screening vs Diagnostic
The same genetic tests can be used for two different purposes. You may opt for a genetic screening test. These tests are for people without symptoms, or to predict risks before pregnancy. However, screening tests don’t prove whether a genetic factor detected causes miscarriage or other pregnancy complications.
To diagnose the cause of miscarriage, your doctor may combine diagnostic genetic tests with symptoms, presentation, and history.
Screening tests are typically safer and more affordable. Whereas, diagnostic tests are often more invasive and more expensive, although more accurate 1.
Parental Screening
Parents may opt for a carrier screening before trying for a baby or early in the pregnancy. It detects chromosomal abnormalities or genetic disease mutations while you don’t have any symptoms. Common genetic diseases that these tests screen for include cystic fibrosis, spinal muscular atrophy, and Tay-Sachs disease.
A karyotype performed on the parents prior to a pregnancy serves as a screening test. Whereas, after a miscarriage occurs, if a parental karyotype is done diagnostically to identify the cause of a miscarriage.
Parental screening test: performed on parents before pregnancy to flag any potential genetic disorders that may arise
Parental diagnostic test: performed after a miscarriage to diagnose the cause of the miscarriage, or rule out genetic causes.
Prenatal (Pregnancy) Genetic Screening
Your doctor may recommend a prenatal screening test early in a high-risk pregnancy to detect genetic abnormalities in the fetus. Pregnancies that are at high risk for genetic disorders may have some of the following factors 23:
- Family history or a previous child with a genetic condition
- Previous miscarriages with known genetic causes or neural tube defects
- A previous stillborn child with apparent signs of a genetic disorder
- If either parent is a carrier for a specific genetic condition
- Abnormal ultrasound findings
- A history of recurrent miscarriages
- You are 35 or older
Recent molecular techniques have made it possible to screen for fetal DNA anomalies from just maternal blood samples. These tests are called non-invasive prenatal testing (NIPT). Some labs or clinics may call them non-invasive prenatal screening or cell-free fetal DNA screening.
However, NIPT may not provide a conclusive diagnosis, requiring further amniocentesis or chorionic villi sampling (CVS) tests.
Non-invasive prenatal testing (Cell-free fetal DNA screening)

NIPT is a non-invasive and affordable screening test for genetic anomalies in the fetus. You only need a blood draw, so it does not present a risk to the fetus.
Can NIPT be wrong?
Currently, the American College of Obstetricians and Gynecologists (ACOG) and the Society of Maternal-Fetal Medicine recommend NIPT only for high-risk pregnancies. Large studies in low-risk groups show that while a negative NIPT test can 100% rule out genetic anomalies, only 30% of positive NIPT tests predict true pregnancy problems. Therefore, these organizations do not recommend NIPT tests for low-risk pregnancies because the positive results may create false alarms 5.
NIPT uses next-generation sequencing technology, which may introduce a high risk of errors in some cases. Therefore, your doctor will interpret NIPT together with other pieces of information, especially before major decisions such as pregnancy terminations. These other pieces of information include 6:
- Symptoms and history
- Amniocentesis or CVS
- Other pregnancy hormone tests (see Double, Triple, and Quadruple Tests below)
NIPT involves analyzing fetal cell-free DNA, which arises from remnant fetal cells that release their DNA into the mother’s blood. This fetal cell-free DNA is typically present in short fragments that can be easily isolated for genetic analysis. Typically, there is enough cell-free DNA concentration in the blood to test for abnormal chromosome numbers after about week 10 of pregnancy 7. The NIPT test can also tell the baby’s gender earlier than an ultrasound test can, with a 1% error rate.
An abnormal NIPT test is usually an indication for amniocentesis or CVS to confirm the findings in the fetus.
Double, Triple, and Quadruple Tests
These tests are not genetic tests per se. They are risk estimations of trisomies 21, 18, and 13 based on a combination data. A double test considers the following 8:
- maternal age – older mothers are at higher risk
- maternal weight, race, and number of fetuses
- the nuchal translucency measurement (NT) based on the appearance of fluid under the skin behind the fetal neck on the ultrasound during the first trimester. The larger NT size, the more probable Down’s syndrome is. A value of >2 mm or >95th percentile for their gestational age is considered abnormal 9.
- gestational age calculated from the crown-rump length (CRL) measurements
- free beta hCG, an elevated number of at least twice the median value could indicate Down’s syndrome 10
- pregnancy-associated plasma protein-A (PAPP-A), value below 0.5 Multiple of Median (MOM) is abnormal.
The triple test also includes alpha-fetoprotein (AFP), which is a protein from the fetal liver. Abnormal levels could indicate a birth defect including neural tube defects and Down’s. However, AFP could also be elevated due to twin pregnancies or miscalculation of due dates 11. The normal range between the 15th – 20th week is 10 – 150 ng/mL 12.
The quadruple test also includes AFP, unconjugated estriol (uE3), and dimeric inhibin A in addition to the blood tests above. This test is done between the 15th – 23rd week, although between 16th – 18th week is better for estimating the risk of neural tube defects 13. Dimeric inhibin A is a protein from the fetal placenta. Elevated levels of twice the median value may indicate Down’s syndrome 14.
The lab will plug in your results into a statistical calculation to determine the probability of birth defects, depending on their reference ranges 15. They may report it as high or low probability, along with a number, such as “1:100000 chance of trisomy.”
Table: Screening tests by gestational weeks and their predictive value 16.
| Tests | Gestational Week | Blood Tests included | Risks detected |
| Double | 10 – 14 | NT, beta HCG, PAPP-A | Trisomies 13, 18, and 21; 70 – 87% sensitive for Down’s, 5% true + false positive rate 17 |
| Triple | 15 – 23 | Beta HCG, AFP, uE3 | 69% sensitive, 5% true + false positive rate |
| Quadruple | 15 – 23 | Beta HCG, AFP, dimeric inhibin A, uE3 | >80% sensitive for Down’s, true + false 5% positive rate |
Each of these sets of tests has limited predictive value, but when multiple of these are combined, the accuracy could be up to 96% 18. However, because the NIPT tests often provide more informative information and have a lower false-negative rate, many clinics prefer to use NIPT as the first screening tool 19. In any case, it will be necessary to confirm the findings with amniocentesis or CVS tests.
Amniocentesis (16 – 18 GW)
Amniocentesis is a collection of amniotic fluid for genetic analysis. Because the fluid surrounds the fetus throughout the pregnancy, it typically contains dissolved fetal cells and DNA 20. This test can also tell about neural tube defects, whereas CVS does not.
Chorionic villi sampling (11-14 GW )
In CVS tests, the chorionic villi are sampled for DNA testing. The chorionic villi are parts of the placenta that allow communication between the mother and the fetus. These villi contain the fetus’s cells 21.
The sample can be obtained through the cervix (transcervical) or the abdominal wall (transabdominal) 22.
The procedures for sample collection are similar for both amniocentesis and transabdominal CVS 23. First, your doctor will perform an abdominal ultrasound to locate the placenta and fetus. Then, they will sterilize the abdomen and insert a thin needle through your abdomen into the uterus to collect the amniotic fluid. You will need to be completely still during this procedure. You may sense minor discomfort and some cramping when the needle enters the uterus.
For CVS through the cervix, your provider will sterilize your vagina with an antiseptic before inserting the catheter through your cervix. When the catheter reaches the placenta, they will use a suction to collect the villi sample.
After the procedure, your doctor will monitor your baby’s heart rate and wellbeing with an ultrasound.
These procedures last 15 – 30 minutes, and you should be able to resume your normal activity after the procedure. Avoid vigorous exercise and sexual activity for a day or two.
Contraindications of transcervical chorionic villus sampling include 24:
- An active cervical or vaginal infection
- Vaginal bleeding or spotting in the previous two weeks
- An inaccessible placenta
Contraindications for transabdominal chorionic villus sampling include a tilted uterus or having a placenta located towards your back 25.
Risks associated with amniocentesis and CVS include 26:
- Leaky amniotic fluid – Amniotic fluid may leak through the vagina after amniocentesis, although this typically stops after one week and the pregnancy will continue normally.
- Miscarriage – Your doctor may explain to you that there is a 0.1 – 0.3% risk of miscarriage from these procedures, depending on the clinic and study they quote. In a large aggregate study, when they compared only among women with similar risk profiles for chromosomal abnormalities, the risk of miscarriage due to amniocentesis is 0.12% and non-existent for CVS 27.
- Rh sensitization – the procedure may expose the baby’s blood cells to the mother’s bloodstream. If the mother has Rh-negative blood and the baby has Rh-positive blood, the exposure may cause the mother to produce Rh antibodies. These antibodies can cause the placenta and damage the baby’s red blood cells.
- Infection or transmission – In very rare cases, an amniocentesis may cause infection. If the mother has an infection, such as hepatitis C, toxoplasmosis, or HIV/AIDS, these procedures can introduce the infection to the fetus.
After these procedures, contact your OB/GYN if you experience28:
- vaginal bleeding or loss of amniotic fluid through the vagina
- Severe cramps that last more than a few hours
- Fever
- Redness and inflammation where the needle was inserted
- Unusual fetal activity or a lack of fetal movement
Preimplantation genetic tests with IVF
Preimplantation genetic tests screen for the chromosomal anomalies in embryos from chromosomally normal parents around 5 days post-fertilization. Your IVF clinic may use a variety of testing methods to select the best embryos before an embryo transfer.
In couples with a known genetic abnormality, a preimplantation genetic diagnostic test can determine if the embryo also inherited the genetic abnormality from the carrier parent. The test can help select for the unaffected embryo.
Some couples use preimplantation genetic tests to select for the gender of the embryo.
Product of conception genetic tests
A miscarriage can be devastating, especially if you don’t know why. The most common cause of early miscarriages is genetic anomalies, so testing the product of conception (POC) typically confirms the genetic cause of the miscarriage. If you have had multiple miscarriages, testing the POC may not only help you understand why but also provides actionable information to improve the chance in future pregnancies 29.
The POC refers to the product of the union between the egg and the sperm. The term also includes a blighted ovum, which has the pregnancy sac but no embryo. Typically, a testable POC sample can be collected from week 8, as earlier POC can be very similar to menstrual bleeding. Your doctor may collect a POC sample before a curettage procedure using a hysteroscope (a thin lighted telescope inserted through the cervix) if you choose to have a dilatation and curettage (D&C), read more about the decision to have a D&C here. If you opt against a D&C, some genetic labs may allow you to collect the product of conception yourself if you can preserve the samples as instructed, although the samples may be of lower quality 30.
Testing the POC with a new technology called the chromosomal microarray (CMA) can significantly improve the success rate of diagnosing the causes of recurrent miscarriages. Currently, the standard diagnostic procedures successfully find the true causes of recurrent miscarriages in only about 45 – 50% of cases. In a small study involving 100 women with recurrent pregnancy loss, testing the POC for genetic anomalies together with the standard workup identified true causes in 95 cases 31!
The chromosomal microarray (CMA, see below for more details) is a more precise way to identify genetic anomalies than karyotyping analysis 32. It can also find smaller genetic variations not otherwise identified with a karyotype 33.
Genetic Testing Technologies for Miscarriage
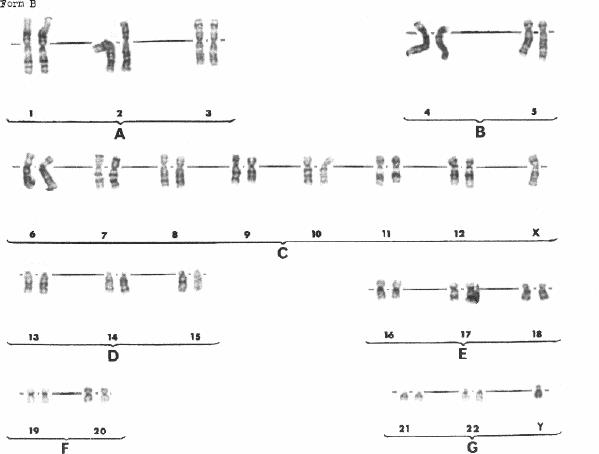
Karyotype Analysis
Karyotype Analysis involves taking a photograph of condensed chromosomes under the microscope. To successfully have a karyotype, the cells have to be dividing cells such as your white blood cells or fetal cells from amniocentesis or CVS.
To see how a lab performs karyotyping, watch the video in this study 34.
A karyotype involves growing the collected cells in the lab, which requires the tissues to be alive. A parental karyotype typically requires a blood draw. For a fetal karyotype, a CVS or amniocentesis procedure can collect the required fetal cells. For a miscarriage POC, sample collection before a D&C procedure may be necessary.
In the lab, the technician will grow the cells to the stage where the chromosomes condense the most before fixing the cells on a glass slide. Then, the cells are burst to spread the chromosomes under the microscope. To visualize specific parts of chromosomes, the technician will apply dyes such as the Giemsa (G-banding) stains, which produces recognizable patterns on each chromosome. Nowadays, there are also other types of dyes and probes that make it easier to recognize each chromosome and easily identify the translocations, if any.
Lastly, the technician will take a photograph of stained chromosomes under the microscope. The images will then be sorted into a karyogram and analyzed 36.
A karyotype can diagnose abnormal chromosome numbers and other chromosomal translocations that are visible under the microscope. These anomalies will have to be large enough (>7 million base pairs) to be visible under the light microscope typically used for a karyotype 37.
Karyotyping is a 50-year old technology with many shortfalls. Because the cells need to be cultured for a karyotype, only live tissues can be used. The culture process is also time-consuming, possibly taking 10 – 21 days 38.
For many couples, the long wait for the test results can be agonizing. Growing the cells in a test tube can also introduce additional genetic errors and chromosomal anomalies. If the cells fail to grow in the test tube, then the karyotype test will fail 39.
Other tests that don’t require cell culture, including non-karyotyping fluorescent in situ hybridization, chromosomal microarray, and next-generation sequencing will bypass these shortfalls of karyotyping.
Fluorescent in situ Hybridization
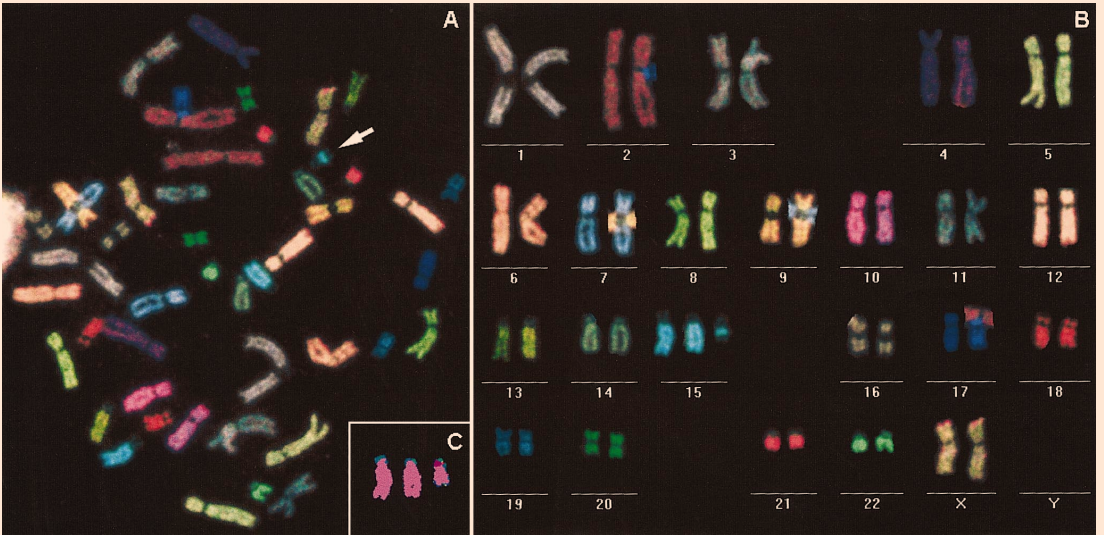
FISH is a technique that tags specific genetic sequences in a chromosome using fluorescent probes. You can do FISH with or without karyotype. The fluorescent probes come in many different colors, which makes it possible to detect multiple types of chromosomal anomalies or genetic variants at the same time. The lab would have to know the genetic sequence of these variants in advance so they can design the probes to target them.
FISH along with karyotyping makes it easier to identify chromosomal translocations and gross abnormalities.
FISH without karyotype does not require cell culture or live cells, so it turns around faster than a karyotype 41. It also does not require a large amount of starting tissue. This test can identify common genetic variants and abnormal chromosome numbers, but cannot identify translocations or unknown chromosomal abnormalities.
Specific clinical utilities of FISH include:
Sperm chromosome testing – Sperms are not dividing cells, so a karyotype is not possible. A FISH test can diagnose incorrect chromosome numbers in ejaculated sperm in men with recurrent pregnancy loss. Based on a study of 140 men with recurrent pregnancy loss, the incorrect chromosome numbers in these sperms don’t correlate with sperm DNA fragmentation (read more in our sperm DNA fragmentation article) 42. Therefore, sperm chromosome testing can provide information that sperm analysis or sperm DNA fragmentation tests cannot.
Preimplantation embryo testing – FISH can identify chromosomal anomalies in unused preimplantation embryos or embryo biopsy. In a small study of 39 embryos, a FISH test identified chromosomal abnormalities in 41% of embryos from three couples with recurrent pregnancy loss 43.
Comparative Genomic Hybridization (CGH)
In Comparative Genomic Hybridization, the lab cytogenetic technician compares two DNA samples for changes in copy numbers. For example, they may label the fetal sample in green and the control sample in red. In the past, the two labeled DNA samples were hybridized to a standard chromosome or cell on a slide before visualizing with a microscope. Now, most CGHs are done using microarrays (see CGH arrays under Chromosomal Microarray).
Chromosomal Microarray
Chromosomal microarray (CMA) is like upgraded karyotyping but with microarray technologies. It can identify chromosomal abnormalities (aneuploidies) as well as a karyotype can. But because CMA doesn’t need to grow the cells in test tubes, it has many advantages over karyotyping, including 4445:
- CMA only requires DNA, so you can also test dead tissue or non-dividing cells, whereas karyotype requires live cells that will grow in test tubes.
- CMA technology can also identify smaller mutations that are not visible on a karyotype. Therefore, you are more likely to find something with CMA than with karyotype.
- CMA does not introduce additional genomic errors from the cell culture process.
- CMA typically has a shorter turnaround time than a karyotype.
- For POC testing, CMA is less susceptible to contamination of maternal materials; it works by comparing a suspected abnormal sample (such as a POC) to a normal sample (such as that of a parent or another healthy person).
- CMA costs less than a karyotype 46
There are 2 types of microarrays, single nucleotide polymorphism (SNP) arrays and comparative genomic hybridization (CGH) arrays.
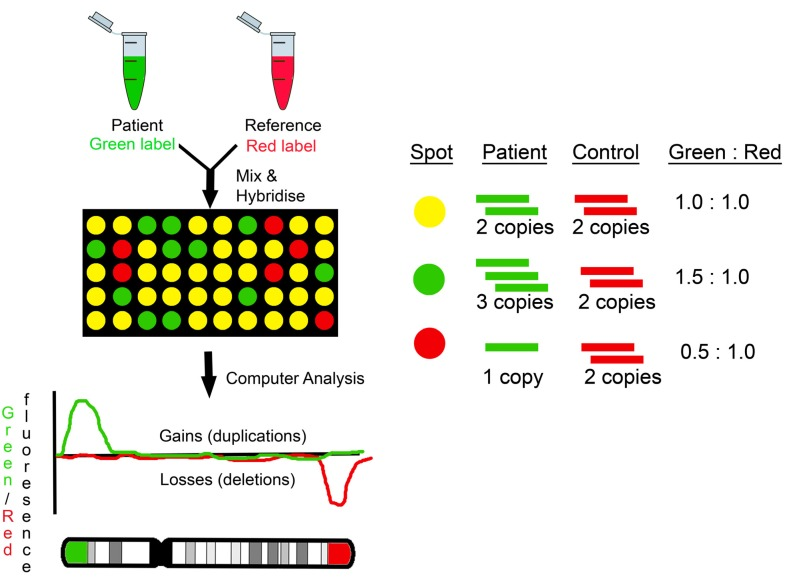
In a CGH microarray test, the lab technicians chemically label patient DNA and normal DNA with fluorescent dyes in different colors, typically in red and green. They then mix the two DNA samples and apply the mixture to a glass slide that has DNA probes printed in a grid. Each of these DNA probes can recognize and bind (hybridize) a small part of your genome. After the binding and rinsing, a fluorescent camera takes a picture of the glass slides. Then, the computer algorithm analyzes the image and measures fluorescent intensity from each DNA probe and compares between two colors. If a color is twice as bright in the patient sample compared to the normal sample, it typically means that that segment of the DNA recognized by the probe is duplicated.
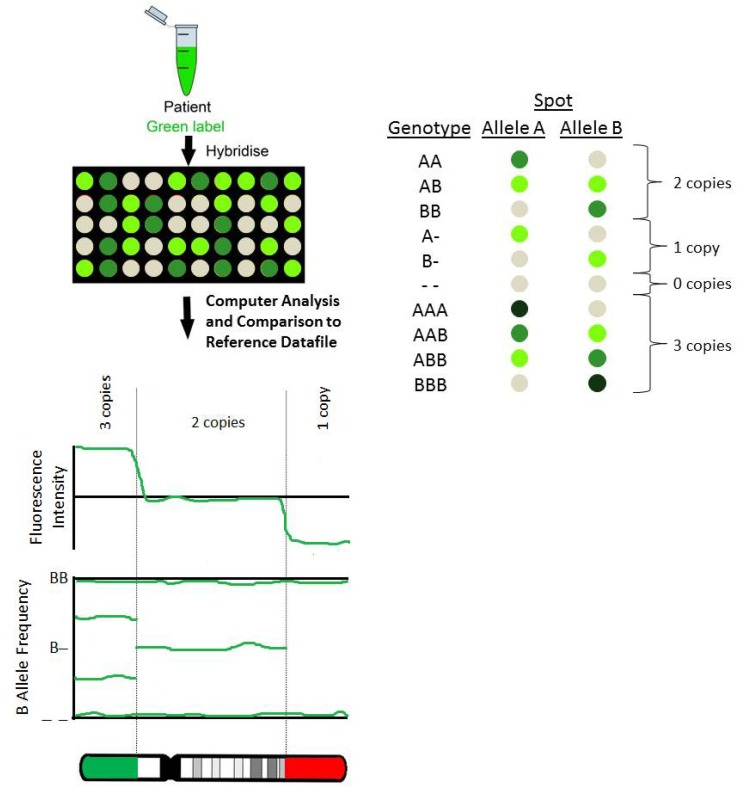
A SNP microarray also has probes recognizing each region of the genome printed on the glass slide, but there are multiple versions of each probe on the grid. Each version of the probe corresponds to a version based on the SNP or single nucleotide change. The total intensity of probes that correspond to a region of the genome can tell if you have a gain or loss of DNA in the region. A key advantage of the SNP array is that it can identify known SNPs in the samples in addition to larger genetic changes.
A microarray mainly measures the relative increase or decrease in DNA throughout the genome. Therefore, it may not detect balanced translocations and chromosomal inversions if there is no net gain or loss of DNA 49. Currently, only a karyotype can detect balanced translocations or inversions without net gain or loss of DNA.
Next-generation sequencing
NGS, also called massively parallel sequencing, is a new technology. NGS has made it possible to determine the genome sequence, either in total or targeted to specific regions of interest. This technology first breaks down the DNA into small fragments, then determines the DNA sequence of all fragments in parallel. Lastly, a computer algorithm compares the data to an existing human genome and scans for anomalies.
NGS is a very new technology with its own flaws. For example, because the sequencing is done in small fragments, sometimes the computer algorithm struggles with telling apart fragments with similar genetic sequences that come from different regions of the genome. Currently, the ACOG does not recommend NGS other than NIPT screening in high-risk cases and research applications 50.
NGS is the main technology for NIPT. It can also be used for carrier screening and testing the POC to identify causes of miscarriage.
An NGS test is like an upgraded microarray. It can provide very similar benefits as a microarray. NGS can determine genetic sequence without prior knowledge,. Whereas, microarray only detects the differences between the DNA sample and the known probes on the microarray. Therefore, NGS can technically identify more types of genetic variations, including translocations and inversions 51. Targeted NGS is a type of NGS designed to specifically look at certain sets of genes or targeted parts of the genome.
Keep in mind that not all genetic variations identified with a microarray or NGS test are problematic. These tests can give you a large amount of information that can be difficult to make sense of 52. Also, if the genetic variation is associated with significant problems, your doctor may order a confirmation test using better-established technology, such as with polymerase chain reaction (PCR) or FISH. If you do get an NGS test, you want to work with a genetic counselor who can help you digest the information and determine your risk and future actions.
Polymerase Chain Reaction
PCR is a molecular technique that makes it possible to identify genetic variants specific to a target genomic region. It is more specific, more precise, and less expensive than NGS. PCR can be adapted to test, screen, diagnose, or confirm the findings in any of the other techniques.
Conclusion
Nowadays, we have better genetic tests than before, and the technologies are rapidly improving. Going through genetic testing may provide closure and also inform you of the best ways to move forward. Newer and more effective tests such as NIPT, CMA, and next-generation sequencing are quickly becoming the standard of care, although karyotyping is still useful. The exciting news is that these new technologies combined with a good workup may identify the cause of miscarriages in over 95% of cases. The key is to know your options so you can seek out the clinics that use these technologies. However, genetic testing is not for everyone so you can always choose not to go through the test or act on the test results.
Next Steps to Consider
- If you are experiencing or have experienced a miscarriage, genetic testing can play an important role in finding answers.
- Use the above information to work with your doctor or other health care professional to fully understand the testing options available to you. If you are interested in newer testing options, don’t be afraid to request these.
- Know that plenty of women who experience miscarriage due to genetic issues go on to have subsequent healthy pregnancies and births
References

0 Comments