

Hi my name is Allison Schaaf, my own fertility journey, including five miscarriages, inspired me to create this website to help you navigate your own fertility journey.
Here are the key takeaways I would share with you as a friend:
- Blood clotting factors are a potential cause of miscarriage and testing may be warranted.
- There are specific protocols that may help with a healthy pregnancy if you have blood clotting issues and have had a miscarriage with blood clots.
- Other than Antiphospholipid Syndrome, blood clotting issues are not always tested/ treated for by doctors, but it may be worth finding a doctor willing to look into it if you have had multiple miscarriages and believe you may have had a miscarriage with blood clots.
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
What Are Blood Clots?
How Do Blood Clots Cause Miscarriage and Pregnancy Complications?
Disorders That Cause Blood Clots During Pregnancy
Diagnosis and Tests of Blood Clotting Disorders That May Cause Miscarriage
Treatments of Blood Clot Disorders
Disorders that increase blood clots (thrombophilia or a hypercoagulable state) may contribute to the 40-50% of miscarriages and other pregnancy complications that are without anatomic, hormonal, or genetic causes1,2. Also, many women with blood clotting predispositions have no symptoms prior to pregnancy because pregnancy increases the risks of blood clots.
It is not universally accepted that blood clotting disorders are more prevalent in women with recurrent miscarriage. Some large studies suggest that inherited thrombophilias are linked with recurrent pregnancy loss, while others don’t. Therefore, some doctors don’t always screen for or treat these disorders 3. Other doctors, however, may empirically prescribe aspirin and blood-thinning drugs for women with recurrent miscarriage.
The majority of studies report that genetic blood clotting disorders are more prevalent among women with recurrent miscarriage 4. In addition, the small studies that analyzed these women are, convincing. For example, two analyzed recurrent miscarriage patients without hormonal, anatomical, and chromosomal causes (179 and 351 women, respectively). They found that 149 out of 179 and 322 out of 351 of these women had one or more blood clotting disorders. In addition, treatment with 81 mg aspirin and unfractionated porcine heparin (a blood-thinning medication) resulted in successful pregnancies in 98% of these women 56.
Many women with these blood clot disorders go on to have successful pregnancies once their conditions are correctly managed 7. This article will cover different blood clot disorders due to genetic causes, along with how doctors typically diagnose and treat them.
What Are Blood Clots?
Blood clotting is a natural process that protects you from bleeding out when you get bruised or cut. The clots typically seal the wounds to stop the bleeding before allowing the immune system to start the repair processes.
Excessive blood clots can clog the blood vessels, leading to heart attacks, venous thromboembolism, and many other issues. Therefore, your body has many checks and balances to ensure that blood clots happen only when warranted, which explains why there are 12 clotting and numerous anti-clotting factors in your blood.
Under normal circumstances, prothrombin is only converted into thrombin when there is an injury or inflammation. Thrombin then cuts fibrinogen into fibrin, the self-polymerizing monomer of fibers that seals the wounds like natural stitches. Then, factor XIIIa cross-links together the fibrin fibers.
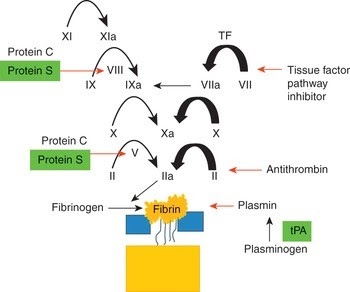
These factors work together in a serial biochemical cascade. Genetic mutations or biochemical disorders that throw off one of these processes can increase the risk of blood clots.
Blood Clotting Changes in Pregnancy
The hormonal and blood changes during pregnancy increase certain clotting factors, making the blood more likely to clot up until childbirth and three months after delivery. Pregnant women are five times more likely to have abnormal blood clots than nonpregnant women. These changes protect women from blood loss during delivery 9.
![How different blood clotting (coagulation) factors change between pregnant and non-pregnant states [5]](https://lh6.googleusercontent.com/1Bh8YYeu2bLiZ87bGL2xFOCqJCEVrejrulJRZEN9kCfz2NA2Tffe7QltN4YHDSmVI1LQKTNOnLtpAB98Rqenz40s3BfiCcxsSOJGq-psIXooDyOpEZssmTWAzjMTrr93A8cjDUaQ)
Source 10
How Do Blood Clots Cause Miscarriage and Pregnancy Complications?
Just as abnormal blood clots cause heart attacks by blocking blood flow to heart tissues, they may also occlude blood flow in the placenta. The occlusion blocks the necessary delivery of oxygen and nutrients to the fetus, which can impair fetal growth and may lead to miscarriage.
Placentation (the formation and arrangement of placenta tissue) and implantation also involve the development of blood vessels and anti-clotting pathways. Therefore, disorders that affect the blood clotting process may cause adverse pregnancy outcomes by interfering with the placentation and implantation processes 11.
Because the placenta starts to take over hormone production and supplying nutrients around 8 weeks, it’s typically only possible to confirm blood clots in the placenta as a cause of miscarriage if it happens around this time. While the 8-week mark is when blood clots can be confirmed via ultrasound or biopsy, blood clots can contribute to earlier miscarriages, but there is no way to confirm.
Blood clotting may also cause other pregnancy complications, including:
- Deep vein blood clots (deep vein thrombosis and venous thromboembolism) where clots may form in the lower body or limbs and may travel to the lungs, causing dangerous pulmonary thromboembolism.
- Preeclampsia
- Intrauterine growth restriction
- Stillbirth
- Placental abruption, when the placenta prematurely separates from the uterine lining
These would all be considered a “miscarriage with blood clots”.
Table: Association of pregnancy complications with blood clotting disorders (+ = possible association, ++ = established association) 12
| Severe preeclampsia | IUGR | Placental abruption | Early recurrent miscarriage (<13 weeks) | Late fetal loss | |
| Antithrombin deficiency | ++ | ++ | + | ||
| Protein S deficiency | ++ | ++ | ++ | ++ | ++ |
| Protein C deficiency | ++ | ++ | |||
| Factor V Leiden | ++ | ++ | ++ | ++ | |
| MTHFR C677T | + | ||||
| Hyperhomocysteinemia | ++ | ++ | ++ | ++ | ++ |
| Factor II G20210A | + | ++ | ++ | ++ | ++ |
| Antiphospholipid syndrome | ++ | ++ | ++ | ++ | ++ |
| Combined blood clotting factors | ++ | ++ | ++ | ++ | ++ |
Disorders That Cause Blood Clots During Pregnancy
Any disturbances that increase clotting or reduce anti-clotting factors in the cascade can increase your risk of blood clots during pregnancy. Interestingly, doctors still disagree on whether blood clot disorders other than antiphospholipid syndrome cause miscarriage because clinical studies of the treatments of these disorders have had mixed outcomes.
Thrombophilia may be inherited due to genetic causes or acquired due to changes in clotting cascades later in life. Keep in mind that it is also possible to have more than one of the causes listed below.
Genetic causes include:
- Antithrombin III deficiency
- Protein C deficiency
- Protein S deficiency
- Factor V mutation
- Prothrombin gene mutation
- Sticky platelet syndrome
Partially inherited causes are a combination of genetic and lifestyle causes, including:
- High levels of factors VIIIc
- Hyperhomocysteinemia, an elevation of homocysteine either from folate deficiencies, MTHFR variants, or other causes
- PAI-1
Acquired causes include conditions developed later in life, such as
- Antiphospholipid syndrome, an autoimmune disease where the body develops antibodies to proteins that are bound to phospholipids, which can lead to blood clots
- Lupus
- Other conditions that may increase blood clots, including blood cancers, cancer, kidney and liver diseases, and inflammatory bowel disease
Factor V Leiden (G1691A and A4044G)
Factor V Leiden is a protein that converts prothrombin into thrombin at the end of the coagulation cascade. Mutations in this gene may significantly increase thrombin production. About 3-8% of people with European ancestry have at least one copy of Factor V Leiden mutation, and 1 in 5,000 people have two copies 13.
Having at least one copy of this mutation is associated with a two- to threefold increased risk of miscarriage, preeclampsia, and intrauterine growth retardation 14.
A4044G increases clotting to a lesser extent than G1691A, but having both can compound the risk 15.
Prothrombin Gene Mutation (Factor II)
Factor II or prothrombin is the last clotting factor in the coagulation cascade. The most frequent mutation in the gene for prothrombin is G20210A. If you have one copy of this mutation, you have a three times greater risk of thrombotic events. If you have two copies, the risk is 20 times 16.
About 2% of caucasians with European ancestry and 0.5% of African Americans have one copy of this mutation 17. It is extremely rare in other ethnicities.
Protein C and Protein S Deficiencies
Factor V activates prothrombin to thrombin. Protein C and Protein S are inactivators of factor V. Deficiencies of proteins C or S may allow the coagulation cascade to overrun, leading to blood clots.
There are 160 different documented mutations in protein C and 330 in protein S. These mutations are associated with increased risk for adverse pregnancy outcomes and up to tenfold increased risk for deep vein thrombosis 18.
Antithrombin III Deficiency
Antithrombin III is a protein that opposes the process of prothrombin to thrombin activation. Lower levels of this protein are associated with increased clot production. It is considered as the most severe out of all congenital thrombophilia clotting defects 19.
It is found in 0.002-0.2% of the US population of all ethnic groups, and around 1-5% in patients with venous thromboembolism 20.
Plasminogen Activator Inhibitor 1 (PAI-1) 4G/5G
PAI-1 is a protein that promotes the prothrombotic state by inhibiting the tissue plasminogen activator. The 4G insertion and 5G deletion variant in front of the PAI-1 gene increases PAI-1 production. The 4G variant may increase the risk of recurrent pregnancy loss by 70%, whereas the 5G variant produces the lowest levels of PAI-1 21.
In a study of 1,032 healthy Italian hospital workers, the 5G variant was found in about 74% of the subjects, making it a relatively common variant 22. Elevated PAI-1 is associated with obesity, metabolic disorder, high cholesterol and triglycerides, and alcohol consumption.
Even without the mutations, PAI-1 may increase with and worsen obesity, metabolic syndrome, diabetes, and some cases of polycystic ovarian syndrome 23,24. PAI-1 levels can be tested directly, although genetic tests for the 4G/5G variants are available.
Sticky Platelet Syndrome
Platelets are cell fragments in your blood that help with blood clots and wound closures. In sticky platelet syndrome (SPS), the platelets aggregate more readily with the presence of adenosine diphosphate (type III), epinephrine (type II), or both (type I) 25.
In a study of 208 patients with infertility and unexplained pregnancy loss, 69 (33.2%) of them had type II SPS 26. Fortunately, SPS responds well to low-dose aspirin therapy, both in terms of cardiovascular risk and reproductive outcomes. Among the 69 women with SPS, 56 of them received low-dose aspirin, 32 became pregnant, and 18 had live births. Whereas among the 13 that did not receive aspirin, 3 became pregnant, and 1 had a live birth 27.
Diagnosis and Tests of Blood Clotting Disorders That May Cause Miscarriage
Blood clotting disorders in pregnancy may be diagnosed with blood clotting tests and Color Doppler imaging with ultrasound.
Currently, the American Society of Reproductive Medicine and the Royal College of Obstetrics and Gynecology do not recommend the genetic tests for thrombophilia listed in this article unless you have a history or family history of thrombotic events 28,29. The main reason is that large clinical studies have not shown clear benefits of treating these conditions for reducing recurrent miscarriage, even though the treating antiphospholipid syndrome with anticoagulants is beneficial 30,31. However, many doctors do empirically test and treat these genetic conditions.
Blood Clotting Tests
These tests can determine if your clotting is abnormal, but they do not specify whether you have one of the genetic mutations that cause it.
- activated partial thromboplastin time (aPTT) indicates how fast your coagulation factors form a clot. The shorter aPTT means the faster clotting time, suggesting that a thrombotic event that may cause miscarriage is more probable.
- Reference range is 30-40 seconds, although on anticoagulant therapy it can be 1.5-2 times longer 32
- D-dimer is a product that forms after fibrinogen degrades, so high D-dimer means there may be ongoing thrombotic processes in your body. However, it is naturally elevated in pregnancy or with other sources of inflammation, so interpretation of D-dimer needs to take these into account.
- Reference range is 0.00-0.49 mg/L FEU
- Anti-factor-Xa is a measurement of heparins in your blood, which can be measured to determine whether the dose of anticoagulants is optimal once the medications are initiated.
- Prophylactic ranges: 0.2-0.5 IU/mL 33
- Therapeutic ranges: 0.5-1.2 IU/ml
Obstetric societies in different countries have somewhat different criteria for thrombophilia testing. These mostly include 34:
- First episode of venous thromboembolism (VTE) at the age of less than 40 years
- Relapsing VTE
- Without varicose veins exhibiting recurrent superficial thrombophlebitis
- VTE in unusual sites (retinal, cerebral, mesenteric or hepatic vein thrombosis)
- Asymptomatic relatives of first-degree patients with proven symptomatic thrombophilia or hematologic disorder that is linked with hereditary thrombophilia
- A history of recurrent unexplained pregnancy losses, fetal growth retardation, or endometrial death
If your doctor suspects you have a coagulation problem, they may order specific genetic testing for mutations in coagulation factors mentioned above, as well as testing for Protein C or S activity levels.
Color Doppler Imaging
Color Doppler imaging is a special kind of obstetric ultrasound imaging where blood flow through uterine blood vessels are assessed. It can detect blood vessel obstructions that could arise from a thrombotic event.
Treatments of Blood Clot Disorders
Blood Thinning Medications
Thrombophilic disorders are usually treated with low molecular weight heparin, such as enoxaparin/lovenox in consultation with hematologists to prevent venous thromboembolism (VTE) during pregnancy. The dosage depends on the patient’s weight and other risk factors. Some patients with no other risk factors may receive only prophylactic doses, while those at an increased risk for thrombotic events require therapeutic doses 35.
| Risk of VTE | Patients | Treatment recommendation by Dr. Kupferminc 36 |
| Very high | – Previous VTE on anticoagulants – VTE in current pregnancy – Antithrombin deficiency |
LMW heparin (Enoxaparin) mg/kg twice/day OR heparin adjusted dose with confirmation of pregnancy |
| High | – Previous VTE – Protein C or S deficiency plus family history of VTE – Homozygote (two copy) Factor V Leiden or prothrombin mutation – Combined thrombophilia |
LMW heparin (Enoxaparin) 40 mg/day until 6–12 weeks postpartum OR fixed-dose heparin |
| Moderate | – Heterozygous (one copy) Factor V Leiden or prothrombin mutation – Protein S deficiency – Family history of VTE |
Postpartum anticoagulation LMW heparin (Enoxaparin) 40 mg/day |
| Relatively low | – Heterozygote FV or prothrombin mutation – No personal or family history of VTE |
Monitor for additional risks for VTE |
Low-dose (Baby) Aspirin
Aspirin is a nonsteroidal anti-inflammatory drug that has a blood thinning effect, so it is often used to prevent heart attacks due to blood clots 37. Because it has been around for a long time, we know a lot about it, and it is available over the counter. Low-dose aspirin is generally safe for pregnancy.
However, aspirin is not free of side effects. It reduces the stomach’s mucous protection, increasing the risk of stomach problems and ulcers. If you are sensitive to salicylates, you may also be allergic to aspirin, so you should inform your doctor in order to get an alternative medication prescribed. Foods that contain salicylates include berries, grapes, plums, cruciferous vegetables, tomatoes, spinach, spices, and tea.
In principle, baby aspirin may improve the chance of successful pregnancy by thinning the blood. However, there are a few studies that focus on women with clotting disorders other than antiphospholipid syndrome.
Studies have confirmed that aspirin and low molecular weight heparin (Enoxaparin or lovenox) improve pregnancy outcomes in the presence of antiphospholipid antibodies 38. For other types of blood clotting disorders and miscarriage causes, however, the research supporting the use of aspirin for miscarriage is unclear.
The Effects of Aspirin in Gestation and Reproduction study tested whether aspirin reduced miscarriage among women who had previously experienced miscarriage. They found no difference between the aspirin and placebo group, except for those who had a single loss before 20 weeks within the previous year 39.
When the same clinical trial was reanalyzed as observational data, they found that using aspirin five to seven days per week led to 15 more live births and six fewer pregnancy losses for every 100 women in the trial 40,41.
In another clinical study, researchers found women with a previous late miscarriage (>13 weeks) who took aspirin had a significantly higher live birth rate but found no difference in women with previous early miscarriage.
The mixed results may be because aspirin helps with some, but not all, causes of miscarriage. It works by thinning the blood and improving blood flow to the uterus, so it likely doesn’t improve the chance of miscarriage due to genetic anomalies or hormonal causes.
Due to the mixed evidence, the American College of Obstetrics and Gynecologists does not recommend aspirin for pregnancies in women with a history of miscarriage or stillbirth 42. However, many doctors empirically prescribe aspirin for women with unexplained recurrent miscarriage based on their clinical experience and each patient’s individual case.
Other Treatments and Management
Blood clotting disorders tend to worsen with increased inflammation, obesity, insulin resistance, and diabetes. Therefore, diet and lifestyle management of these factors may improve pregnancy outcomes.
Elevated homocysteine, which is often caused by folate deficiency, can compound with other elevated blood clot risks. See our homocysteine and MTHFR articles for testing and reducing homocysteine levels.
If you are on blood thinners, watch out for supplements that may interact with these medications. Some of these supplements include vitamin K, fish oil, and systemic enzymes. Always check with your doctor and pharmacist before introducing supplements, especially during pregnancies.
Conclusion
Inherited and partially inherited blood clotting disorders are associated with miscarriage. While the clinical evidence for diagnosing and treating them for recurrent miscarriage has been mixed, many doctors do test and treat these disorders based on their clinical experience. If you’ve had multiple miscarriages, speak to your doctor about getting screened for these blood clot disorders.
Next Steps to Consider
- Many women report suspecting a “miscarriage with blood clots.” In order to learn more, request your doctor test for blood clotting factors, especially with recurrent pregnancy loss (RPL)/ multiple miscarriages.
- Ask your doctor if a protocol to address potential clotting issues is appropriate for you.
- Read our article on Antiphospholipid Syndrome (APS).
References
0 Comments