

Hi, my name is Allison Schaaf. My own fertility journey, including five miscarriages, inspired me to create this website to help you navigate your own fertility path.
Here are my main takeaways I would share with you as a friend:
- Luteal phase defect is not always recognized as an issue when it comes to miscarriage. This article will go into detail on differing opinions on this matter.
- Tracking and understanding your cycle, including your progesterone levels, is an important step towards taking control of your fertility.
- Low progesterone may not be a cause but rather a symptom that correlates to miscarriage.
- However, supplementing with progesterone in certain cases may help to prevent miscarriage.
I also recommend you do your own research and work with your doctor. That is why I have coordinated these articles with the nitty-gritty details and links to research so you can make an informed decision on what works best for you… read on for more! And—don’t miss my Next Steps section at the bottom.
Get a FREE downloadable, printer-friendly version of this article when you sign up for our newsletter, Click HERE.
What is luteal phase defect and what causes it?
Alternative and innovative tests that may diagnose and guide treatments for luteal phase defects
Luteal Phase Defect Natural Treatments: Naturopathic and Functional Medicine Approaches
Other alternative and natural treatments that may lengthen luteal phase defects and increase progesterone
Luteal phase defect and low progesterone seem to be a controversial topic with unclear diagnostic criteria and treatment protocols.
The evidence so far has been puzzlingly mixed, with a lot of controversy about:
- What a luteal phase defect really means
- Whether low progesterone levels or short luteal phase is a problem
- How to diagnose or treat luteal phase defect to prevent repeat miscarriages
In Part 1, Progesterone, we introduce the background info about profgesterone, progesterone therapy, and factors linked to low progesterone.
This article, Part 2, will share with you the background info about luteal phase defect and pregnancy. Then, we’ll discuss the current state of the evidence, along with both conventional and natural options for addressing luteal phase defects in recurrent miscarriage.
What is luteal phase defect and what causes it?
Luteal phase defect (also called luteal phase deficiency) occurs when the uterine lining cannot develop sufficiently to support a pregnancy. This could be due to:
- Insufficient progesterone levels
- Too short of a luteal phase so the uterine lining hasn’t had enough time to properly develop
- Abnormalities in the development of the uterine lining
- Abnormalities of the ovaries or follicles
It may affect 3-4% of infertile couples 1.
Luteal phase defect may not be a problem with the ovary per se, but is rather connected to abnormal pituitary hormones. Luteal phase defect may also be associated with low follicle-stimulating hormone (FSH), low follicular phase estrogen, altered FSH/LH ratios, and abnormal FSH/LH secretions. These conditions reduce luteal phase estrogen and progesterone levels 2.
According to Dr. Aumatma Simmons, MS, ND, FABNE of Holistic Fertility Institute, low luteal phase progesterone reflects poor egg and follicle quality because the egg and follicular cells develop together before the follicles become the corpus luteum.
Progesterone resistance, found in endometriosis and PCOS, can also contribute to luteal phase defects 3 4. Some women’s endometrial linings are less responsive to progesterone. This may reduce fertility.
Symptoms of luteal phase defect may include:
- Spotting during luteal phase
- Shorter cycle length and more frequent periods
- Difficulty conceiving, infertility, and miscarriage
- Shorter luteal phase (<9-11 days)
- Inconsistent increase in basal body temperature (your lowest body temperature at rest) during luteal phase
The absence of basal body temperature rise is not reliable proof that your progesterone level hasn’t increased. Keep in mind that numerous factors change your body temperature, including living habits, exercise, fever, lack of sleep, stress, and alcohol 5. Also, temperature rise for ovulation detection is only accurate in approximately 22% of cases 6.
Other symptoms of low progesterone may include:
- Bloating
- Headaches
- Breast swelling, pain, and tenderness
- Premenstrual syndrome
- Mood and mental health issues, such as anxiety, depression, and irritability
- Weight gain
- Libido changes
- Food cravings
- Sleep problems
- Constipation
However, it’s possible to have low progesterone with no symptoms at all.
If you have these symptoms, discuss them with your doctor, so they can evaluate you for low progesterone.
How is luteal phase defect diagnosed?
Currently, there are no official diagnostic criteria for luteal phase defect. However, if your doctor does monitor it, they may do it with a transvaginal ultrasound or endometrial biopsy.
Transvaginal ultrasound to look at endometrium thickness
During your luteal phase, your doctor may use transvaginal ultrasound to visualize the corpus luteum in one of your ovaries to confirm you’re in the luteal phase. Then, they will look at your endometrial thickness. The endometrial thickness is typically visible during your luteal phase and up to 5 weeks of pregnancy before the embryo and gestational sac become visible.
Alternatively, a blood test for luteinizing hormone and peak progesterone may indicate the right time to check for endometrial thickness 7.
Your endometrial thickness is a good indicator that progesterone is doing its job to help the uterus prepare for implantation. A well-prepared endometrium is called a triple line endometrium.
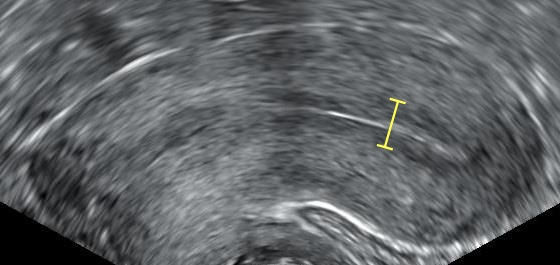
Image caption: Triple-line endometrium on the ultrasound. Source: Wikimedia Commons
Endometrial biopsy
Some reproductive medicine doctors may diagnose luteal phase defects with an endometrial biopsy. Similar to a Pap smear, your doctor will insert a speculum to visualize the cervix. Then, they will use a pipelle, a thin suction instrument, to collect the uterine lining in multiple spots.
The samples will then be placed in a preservative and sent to a pathology lab to examine for thickness and growth patterns.
Why is luteal phase defect controversial?
Reproductive medicine organizations and doctors disagree on whether luteal phase defect is a real issue.
Here are the reasons:
- Several clinical studies show many women can get pregnant despite having LPD 8.
- There seems to be no optimal progesterone level for pregnancy and miscarriage prevention. The idea that low progesterone can cause miscarriage is very controversial. In animal studies, low progesterone levels have been sufficient to maintain pregnancies. Also, progesterone effects on the endometrium are highly modifiable by local factors in the uterus.
- Progesterone is secreted in pulses, so your serum progesterone levels can vary by up to six-fold within a few hours 9.
- There is no accepted treatment protocol for luteal phase defects that will consistently make a difference.
- Like natural killer cells, low progesterone may not be a cause but rather a symptom that correlates with poor pregnancy outcomes 10.
Still, many doctors find progesterone helpful for imminent miscarriage and prescribe it empirically. This practice is based on a logical presumption that progesterone has many important roles in pregnancy, and lower progesterone might cause bleeding in the beginning of the pregnancy 11 12.
Alternative and innovative tests that may diagnose and guide treatments for luteal phase defects
Blood progesterone levels alone may not be indicative of progesterone function, as many factors determine the effects of progesterone function. These include the local uterine environment, progesterone resistance, and even inflammation levels.
Therefore, precision and individualized medicine approaches may work better to boost progesterone function and address luteal phase defects.
Many functional medicine doctors or integrative fertility specialists may use these tests to guide their treatment protocols. Given that many lifestyle factors influence progesterone and luteal phase, many women may get better results through this approach.
Salivary progesterone and steroid hormone panel
Progesterone is secreted into the blood in pulses, so that its levels can vary widely in the span of a few hours, making blood progesterone unreliable. Salivary hormone levels reflect hormone levels in the fluid between cells, which correlate with free or functional hormone levels. Also, salivary hormone levels represent the average of pulses across a few hours.
Salivary collection is non-invasive—you can simply spit into collection tubes. Then, samples can be stored in the freezer, making it possible to collect multiple times a day or on multiple days within the same cycle before sending the samples off to the lab. Many labs also have test kits that allow for testing levels of estrogen and progesterone multiple times during a menstrual cycle.
Therefore, salivary hormone tests, especially for the entire menstrual cycle, may be more clinically meaningful in terms of luteal phase defect and overall reproductive health.
Ishikawa et al. (2002) studied salivary progesterone levels in 121 women. Compared to women with healthy luteal phase, those with luteal phase defect had significantly lower salivary progesterone between days 3 and 10 of their luteal phase.
The authors concluded that the cutoff of 189 pmol/L of salivary progesterone in the mid-luteal phase could correctly diagnose 78% of luteal phase defect cases. Whereas, higher levels can correctly exclude luteal phase defects 76.5% of the times 13.
Gandara et al. (2007) mapped the cycles of 22 women aged 19-40 years. The data demonstrated clear differences between normal, likely normal, and abnormal fluctuations of estrogen and progesterone. These patterns are likely more clinically meaningful than day 21 serum progesterone levels 14.
A small Finnish study examined 46 women with previous miscarriages and 12 healthy controls. Eight of the previous miscarriage group had luteal phase defect, as defined by delayed endometrial maturation as diagnosed with uterine biopsy. However, this study did not detect a statistically significant difference between salivary progesterone levels between the three groups 15. However, one problem with this study was that the 46 women in the miscarriage group included miscarriages from many causes rather than luteal phase defect alone. So, this study may not exclude the possibility that salivary progesterone can be indicative of luteal phase defect.
Another study examined salivary progesterone and estrogen levels weekly from week 24 in women at high risk of preterm delivery. Twenty-eight of them had spontaneous onset of labor and delivery before week 37, compared to 64 who delivered at term.
Women who delivered before 34 weeks had significantly lower progesterone than those who delivered between weeks 34-37 and those who delivered full term. This suggests low salivary progesterone during pregnancy may predict earlier delivery and/or indicate the need for progesterone supplementation 16.
Although salivary progesterone testing has been around for decades, and there are many clinical studies evaluating its usefulness, it is currently not a standard of care for diagnosing luteal phase defects. There is also very limited evidence related to its usefulness to understanding recurrent miscarriage.
Most importantly, salivary progesterone and steroid hormone panels require clinical skills to interpret and treat, so you should always consult the appropriate provider about your results.
Urinary hormone panel, such as Dried Urine Test for comprehensive hormones
Urine hormone tests measure the hormone metabolites secreted by your hormones. If all the metabolites are tested, the test results will show the precursor, metabolism, and breakdown of hormones, including whether some hormones are converted into toxic or cancer-causing versions.
Some people may have more of certain progesterone metabolites than others, so this test provides more illuminating snapshots. Having more of certain metabolites or breakdown byproducts may also indicate some nutrient deficiencies that can be easily corrected.
Dried urine tests involve collecting your urine on a piece of filter paper before drying it off and sending the dried paper to the lab. While these samples may be cumbersome to collect, the tests are non-invasive and can be collected as often as necessary 17.
Urine progesterone reflects the average progesterone levels since the last bladder void. This typically represents a period of one to two hours or longer. When the samples are collected from first morning urine, they typically reflect overnight progesterone levels, which are useful for indicating the day’s progesterone production 18.
The use of urine hormone tests for troubleshooting the menstrual cycle has become more popular lately, but it’s still relatively new. Many of our holistic practitioner colleagues have found great results using these tests for fertility and recurrent miscarriage. However, it may be years or decades before large clinical trials confirm their clinical anecdotes.
At-home progesterone and fertility monitoring tests
Proov and Oova are examples of a at-home urine tests that measures luteinizing hormone and progesterone levels. It’s helpful for predicting the most fertile window and confirming ovulation.
Luteal Phase Defect Natural Treatments: Naturopathic and Functional Medicine Approaches
Naturopathic and functional medicine approaches to fertility typically involve diet and lifestyle changes. Although these approaches can be safe and effective, it is difficult to design and conduct clinical trials to assess their efficacies.
Therefore, we asked Dr. Aumatma Simmons, a naturopathic endocrinologist who specializes in recurrent miscarriage, to share her clinical approach and observations related to pregnancy outcomes.
According to Dr. Simmons, luteal phase defect appears to be a buzzword that may not mean much on its own and may not be a real diagnosis. The key observations include shortened luteal phase, low progesterone, and spotting, so she investigates and addresses the following:
1. Estrogen dominance
She maps the cycle using a full-cycle DUTCH Complete test. Many women have high estrogen during their luteal phase, which could lower progesterone. In this case, we will support estrogen detoxification first. If the progesterone is low, she then looks at egg quality.
2. Low egg quality
Corpus luteum functions are tied to egg quality because the eggs and follicular cells develop together before the follicular cells become the corpus luteum. Therefore, low luteal phase progesterone reflects low egg quality. Mid-luteal progesterone of under 5 ng/mL reflects low egg quality, whereas over 15 ng/mL is optimal for egg quality and fertility.
So, she recommends natural approaches to improve egg quality. These may include addressing:
- Chronic inflammation
- Sources of oxidative stress such as alcohol, smoking, unhealthy diet, lack of exercise, and obesity
- Deficiencies of nutrients and dietary antioxidants
3. Stress
Excess mental and physical stress can increase cortisol and thereby reduce progesterone. Therefore, Dr. Simmons coaches her patients through addressing these sources of stressors. She may also recommend adaptogenic herbs to support the stress response axis.
Low-carb diets can stress the body, potentially causing luteal phase defects or amenorrhea in some women 19.
Healthy sleep and circadian rhythm are also essential for normalizing the stress response. The DUTCH test provides a good snapshot of your circadian rhythm and morning cortisol awakening response.
Some of her colleagues use wearables like the Oura Ring to help monitor the heart rate variability and stress scores.
Herbal support for menstrual cycles and luteal phase defects
In addition to addressing lifestyle factors, Dr. Simmons also uses two herbal formulations—one to support the follicular phase and another to support progesterone production during the luteal phase. The luteal phase formula contains Vitex, which is a progesterone support herb. Because there is limited evidence regarding the safety of herbs during pregnancy, she takes her patients off the herbs before pregnancy.
How effective is natural luteal phase defect treatment for miscarriage?
Overall, low progesterone and luteal phase defects indicate the body’s unreadiness to support a pregnancy, which explains why many of Dr. Simmons’ clients couldn’t get pregnant before.
After following her program and addressing any lifestyle factors affecting the luteal phase, and factor in the male partner, her clients almost always become pregnant and carry the pregnancy to full term.
In her practice, up to 90% of male partners in recurrent miscarriage couples came with blood sugar problems and elevated homocysteine, which contribute to the miscarriage. Fortunately, these are easy to address naturally.
How long does it take to resolve luteal phase defects naturally?
Dr. Simmons’ clients stay on the lifestyle changes and herbal protocols for 2-3 months to lengthen their luteal phase to 12-14 days and normalize their basal body temperature. After that, they have a higher chance of conception and healthy pregnancy.
Other alternative and natural treatments that may lengthen luteal phase defects and increase progesterone
Vitamin C
Henmi et al. (2003) studied 122 patients with infertility and luteal phase defects based on peak progesterone level <10 ng/mL. Seventy-six patients in the study group received 750 mg of vitamin C per day. The vitamin C group had a significant increase (~5-6 ng/mL) in progesterone level and 25% of them became pregnant with a miscarriage rate of 15.8%. Whereas, 10.9% of the control group became pregnant with a miscarriage rate of 20% 20.
Vitamin B6
Vitamin B6 is important for overall steroid hormone function 21. A meta-analysis suggested that 100 mg of B6/day may help with PMS and premenstrual dysphoric disorder, which are associated with low progesterone 22.
Vitex agnus cactus (chasteberry or chaste tree)
Historically, herbalists and midwives used Vitex to prevent miscarriage due to low progesterone. The herb may boost corpus luteum function and affect LH function while reducing prolactin levels 23.
A few clinical studies show that this herb can increase mid-luteal phase progesterone and normalize shortened luteal phase. It may also reduce serum prolactin and help with breast pain and premenstrual syndrome 24.
Despite its historical use, there is very limited evidence for its safety during pregnancy 25. Therefore, you should consult your doctor or midwife before using Vitex.
According to Dr. Aumatma, Vitex should be only used during the luteal phase and stopped during follicular phase in normally cycling women working to improve their fertility. However, in cases of irregular cycles, Vitex may be used continuously.
However, if you struggle with irregular cycles, you may also use Vitex during all phases of your cycle.
Traditional Chinese Medicine
Traditional Chinese medicine (TCM) views luteal phase defects as depleted kidney Qi. Also, different phases of the menstrual cycle correspond to different Qi flow patterns. So, TCM treatments involve restoring these healthy Qi flow patterns.
A clinical study examined 60 infertile women due to luteal phase defects who were treated with herbs to tonify the kidneys and regulate the menstrual cycle. The treatment significantly increased the basal body temperature scores. After the treatment, 32 of these women became pregnant 26.
Another Chinese study evaluated 53 patients with luteal phase defects receiving different herb protocols at different phases of their cycle. After three menstrual cycles of treatment, their luteal phase endometrium significantly improved, their rise in basal body temperature became more consistent, and their temperatures stayed elevated for longer.
Also, while LH and prolactin significantly decreased, progesterone levels increased. These hormonal changes are good for fertility. In the study, 22 of the 53 (41.5%) women became pregnant, but 15 (28%) of them required interventions to keep the pregnancy 27.
Other treatments using acupuncture, moxibustion, and other herbs such as Unkei-to have also been reported to improve progesterone levels and help with infertility due to luteal phase defects 28 29.
Low-level laser therapy
Low-level laser therapy (LLLT) refers to brief applications of red (600-660 nm) or infrared light (800-880 nm) either for the entire body or specific regions, such as the uterus. These specific light spectra can activate the mitochondria, which has an anti-aging effect. The treatment lasts from a few seconds to 20 minutes. It’s generally a very safe and non-invasive procedure with few to no side effects.
Several clinical and preclinical studies suggest that red light therapy may help with fertility and luteal phase defects. However, there is no evidence that it helps with miscarriage.
Low-level laser therapy may help with fertility by boosting mitochondrial function and reversing cellular aging. In a clinical study, 156 out of 701 women who had failed fertility treatments became pregnant after receiving 830 nm LLLT treatments. The live birth rate in this study was 50.1% 30.
In an animal study, 660 nm infrared seemed to increase serum estrogen and progesterone levels 31. Another animal study showed that it reversed ovarian aging, although it reduced follicular phase progesterone 32.
Note: This article may contain affiliate links. We appreciate your support of Miscarriage Hope Desk!
Next Steps to Consider
- Ask your doctor if you think you may be experiencing low progesterone or luteal phase deficiency.
- If you are not already, begin tracking your cycles and basal body temperature using tools like TempDrop (use this link to save 10% at checkout).
- In addition to tracking your cycles, consider testing your progesterone levels. There are multiple at-home tests like OOVA (use this link to save 10% at check out) and Proov. We recommend also working with a medical professional to interpret your results!
- Download our free lab checklist for more testing to consider if you are experiencing recurrent miscarriages.
- Sign up for our newsletter, here, and receive a FREE pdf of this article.
References

0 Comments